

As women in medicine, we are always focused on the next goal we need to achieve to advance our career. Through undergraduate education, medical school, residency, and fellowship, we are constantly striving to get the highest score, to maintain a high GPA, to publish papers, to get excellent letters of recommendation. The challenge that women physicians face is balancing these demands in the midst of our passing prime reproductive years. We plan a trajectory of our career from an early stage, sometimes as early as our undergraduate years. But do we have the same foresight about an equally important part of our life journey: planning for a family?
Infertility affects 1 in 8 couples in the general population, however infertility affects 1 in 4 women physicians (1). There is never a good time to have a family in our training years or in our early post-training years for that matter. But, if having biological children is important to us, this must be something we think about in advance.
Here are some general infertility facts and statistics that are helpful to know:
- Each month, a young woman’s chances of conceiving is about 20-30%, assuming the woman has regular cycles and no known causes of infertility. This percentage starts to drop slightly at age 32, and more significantly at age 35. The chance of success declines with increasing age and increasing duration of time of trying to conceive without a successful pregnancy.
- We are born with a certain number of eggs, and this number declines with time. Women cannot regenerate eggs, while men can regenerate sperm. So once the pool of remaining eggs is low, there is nothing we can do to increase our remaining egg supply.
- As the female partner’s age increases, so does the chance of miscarriage. In our 20’s, the miscarriage rate is approximately 12-15%. Between ages 35-39, the miscarriage rate increases to approximately 20-30%. After age 40, the miscarriage rate approaches 50%.
- As females age, there is an increasing proportion of genetically abnormal eggs (from meiotic nondisjunction) leading to the observed decreased pregnancy rates and increasing miscarriage rates.
These statistics can be sobering, especially as more professional women continue to delay starting their family whether it is by choice to pursue their career or if it is because they have not found the right partner. A study looking at childbearing patterns and decision-making among American physicians found that females doctors with infertility stated if they could go back and do things differently, some would have started a family earlier, gone into a different specialty, undergone treatments to preserve their fertility, and some would have not done anything differently (1). Knowing about fertility and timelines early is key, so that we can make decisions on what is right for each of us individually and so that we do not regret the choices we made later.
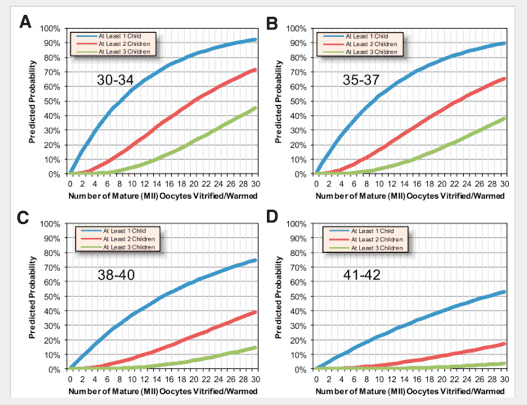
Egg freezing is the process of cooling eggs to sub-zero temperatures to preserve reproductive potential. This technology may allow women to have the opportunity to have biological children later in life, but there are limitations. First, freezing eggs is not a guarantee for a biological child. It is an option that gives us some control over increasing the chances of having a biological child in our more advanced years, which we did not have before. The ideal number of eggs that a woman should consider freezing is dependent on many different factors: the woman’s age, her ovarian reserve, the number of children she wants to have, the likelihood of live birth that she is comfortable achieving, and the number of IVF cycles she would like to undergo. While more and more women are pursing egg freezing, there still hasn’t been enough time to allow a significant proportion of these women to come back, thaw their eggs and attempt to have a child to provide better estimates of the success rates at various ages. Therefore, the data is limited on live birth rates per egg, especially in older women. With that caveat, there are a few studies reporting prediction models that can provide some guidance on the chances of having a live birth based on a woman’s age at time of egg retrieval and number of mature eggs cryopreserved (Figure 1) (2). To briefly summarize, freezing 15-20 mature eggs for women <38 years old gives them approximately 70-80% chance of at least 1 live birth. For women 38-40 years old, freezing 25-30 mature eggs gives them roughly a 65-75% chance of at least 1 live birth (2). Sometimes we can retrieve 10-15 eggs in women <38 years old from 1 IVF cycle, but sometimes it requires more than 1 cycle. The number of eggs retrieved from each IVF cycle is ultimately dependent on each individual woman’s circumstance: her age and her ovarian reserve, which is in large part genetically predetermined. Generally speaking, the younger a woman is, the better her chances at retrieving a larger number of better quality eggs with less IVF cycles. The disadvantage, however, to freezing eggs at a younger age is that the woman may not end up using these cryopreserved eggs. Conversely, the older the woman is, the more likely it is to undergo more IVF cycles in order to freeze more eggs of lower quality to achieve comparable pregnancy rates. Therefore, if a woman is considering egg freezing, a good time to start thinking about egg freezing is in between these two extremes in your early to mid-thirties (ie ages 32-37 years old).
The process of egg freezing usually overall takes about 2 months to complete and involves 3 steps: 1) the workup, 2) ovarian stimulation, and 3) an egg retrieval.
Step 1:
You will see a Reproductive Endocrinology and Infertility (REI) Specialist. They will take a detailed history, do a physician exam, and perform a transvaginal ultrasound. They will also do an assessment of ovarian reserve (a term used to reflect remaining egg supply and fertility potential a woman has). There are 3 tests for ovarian reserve: 1) antral follicle count (AFC), 2) antimullerian hormone (AMH), and 3) day 3 FSH (follicle stimulating hormone). Once we have these test results, the REI will meet with you again to go over these values and expectations prior to undergoing stimulation. The patient will also meet with an IVF nurse to discuss a calendar and go over medication teaching.
Step 2:
Ovarian stimulation refers to stimulating the growth of ovarian follicles, which contain an immature egg within it. The process starts with either birth control pills for 2-3 weeks or estrogen for 1 week. This will help synchronize the follicles to grow together so we optimize the number of eggs we are able to retrieve. Then, a patient will undergo 10-12 days of injections to stimulate the ovarian follicles. Each day involves injecting 2-3 medications in the stomach or thigh subcutaneously. Some common side effects of the medication include: bloating, abdominal discomfort, sometimes mood swings, and local bruising at the injection site. During this time frame, patients will get bloodwork and transvaginal ultrasounds performed every 2-3 days, for a total of usually 4-5 visits. Once the follicles reach the appropriate size, the patient will do a trigger injection, which induces the final stages of egg maturation. The egg retrieval will then be scheduled 35-36 hours after the trigger.
Step 3:
The egg retrieval is a minor surgical procedure that is performed under conscious sedation. Under ultrasound guidance with a small needle and gentle vacuum suction, the follicles are drained of all the fluid within them. The procedure usually takes about 15-20 minutes. The fluid is then given to the embryologist who will look for the eggs in the fluid. They will then assess the eggs for maturity, and freeze all of the mature eggs. The most commonly performed type of freezing method is vitrification, a process using an ultra-rapid cooling technique to solidify the cell into a glass-like state. Compared to the previous slow freezing method, vitrification has been shown to decrease the formation of ice crystals (which can damage the egg) and has improved the overall success rates of freezing eggs. After the egg retrieval, some cramping and light bleeding are normal, but generally resolve quickly and patients are often feeling back to normal 1 to 2 days later.
After the entire process is complete, patients will often meet with their REI again to review the outcome of the cycle. Based on the number of mature eggs frozen, we can assess if we met out goals with that cycle or see if another cycle is needed or desired.
Fertility lasts for a finite period of time, so it’s important to prioritize thinking about it. Take control of the information available, learn about what advancing age does to fertility, check your ovarian reserve, learn about treatment options available, and make a plan that is right for you, just as you do with your career path. The ultimate plan may be to start a family earlier, to freeze eggs or embryos, or to not make any changes because we are comfortable with alternative means of having a family such as donor egg or adoption. Every woman has their own unique path to building a family. Ultimately, I would urge women physicians to make informed decisions early on regarding planning a future family, and not allow the passage of time to make the decision for you.
This article was originally published on SheMD.org
Anu Kathiresan, MD is a practicing Fertility Specialist at Center of Reproductive Medicine in Houston, Texas. She’s the Director of Fertility Preservation and Patient Education. She has fertility educational video series called “Fertility Friday” which can be found at www.bit.do/anukathiresanmd. She also can be followed on Instagram, Facebook, and YouTube @anukathiresanmd.
References:
1) Stentz NC, Griffith KA, Perkins E, Jones RD, Jagsi R. Fertility and Childbearing Among American Female Physicians. J Womens Health. Oct 2016; 25 (10): 1059-1065.
2) Doyle JO, Richter KS, Lim, J, Stillman RJ, Graham JR, Tucker MJ. Successful elective and medically indicated oocyte vitrification and warming for autologous in vitro fertilization, with predicted birth probabilities for fertility preservation according to number of cryopreserved oocytes and age at retrieval. Fertil Steril. Feb 2016; 105 (2): 459-66.



