
What exactly is trauma-informed care?
Doesn’t everybody deal with bad things in their lives? Why should we dwell on trauma? Is it really that big of a deal? Shouldn’t people ideally find their own ways to cope?
The mission of pediatricians and pediatric primary care providers is to promote the health of children and their families and to advocate for their wellbeing. Pediatricians, and ANYONE in the health professions should see these adverse experiences as a big deal, as they can affect all of us “for good”. Forkey emphasized in the American Academy of Pediatrics (AAP) clinical report that, though their mission is consistent with becoming trauma-informed, pediatricians often lack the tools they need to benefit this growing population under their care.

The need for a new approach to prevention, identification and therapy around childhood trauma and child traumatic stress is urgent. Nearly half of American children, or 34 million people in the US younger than age 18, have faced at least one potentially traumatic early childhood experience. (Forkey, 2021). Examples of traumatic childhood experiences include community violence, natural disasters, unintentional injuries, terrorism, immigrant or refugee traumas (including detention, discrimination, or racism), bullying, and/or those involving the caregiving relationship, such as intimate partner violence, parental substance use, parental mental illness, caregiver death, separation from a caregiver, neglect, or abuse.
We increasingly are learning about the long term effects of these events. There are measurable physiologic consequences of accumulated trauma experiences on both the brain and the body (immune and endocrine systems). These consequences can impact children’s health acutely and can persist throughout adulthood.
It’s important for healthcare providers of all types to recognize those adults who have experienced unmitigated traumatic early childhood events who present to every type of healthcare setting. They may be having symptoms or behaviors consistent with consequences of trauma that have not been fully identified as precursors to their presenting problem.
A trauma-informed approach allows us to develop the skills and mindset we need to fully understand, respect, and advocate for the health of our patients and families, our coworkers, and ourselves..
The pnemonic “FRAYED” depicts symptoms that may occur as a result of trauma early in life. Another common but overlooked type of trauma in children revolves around having been treated or having undergone medical procedures for a potentially life-threatening illness, called “Pediatric Medical Traumatic Stress” or PMTS.
Most Common Symptoms of Trauma Exposure
F Frets (anxiety and worry) and fears
R Regulation difficulties (disorders of behaviors or emotions; hyperactive, impulsive, easily becomes aggressive or emotional; inattentive)
A Attachment challenges (insecure attachment relationships with caregivers); poor peer relationships
Y Yawning (sleep problems) and yelling (aggression, impulsivity)
E Educational and developmental delays (especially cognitive, social-emotional, and communication)
D Defeated (hopeless), depressed, or dissociated (separated from reality of moment, lives in own head)
Adapted from Forkey H, Griffin J, Szilagyi M. Childhood Trauma and Resilience: A Practical Guide. Itasca, IL: American Academy of Pediatrics; 2021.
Trauma-informed care is defined as medical care in which all parties involved assess, recognize, and respond to the effects of traumatic stress on children, caregivers, and health care providers. (Forkey, 2021) This type of care fosters a nonjudgmental approach, encourages resilience, and enlists caregivers to be engaged (two generation approach). It can provide an explanation for struggles and perhaps perplexing and stress-inducing behaviors affecting a person’s and family’s health and well-being. The psychological literacy and education promoted in a trauma-informed model of care can help empower all involved to become more resilient. There are five components of trauma-informed care outlined in the clinical report:
- Awareness
- Readiness
- Detection and Assessment
- Management
- Integration
This topic isn’t typically well-known to practicing clinicians. I encourage you to dive more deeply into the references I’ve provided for a more comprehensive understanding.
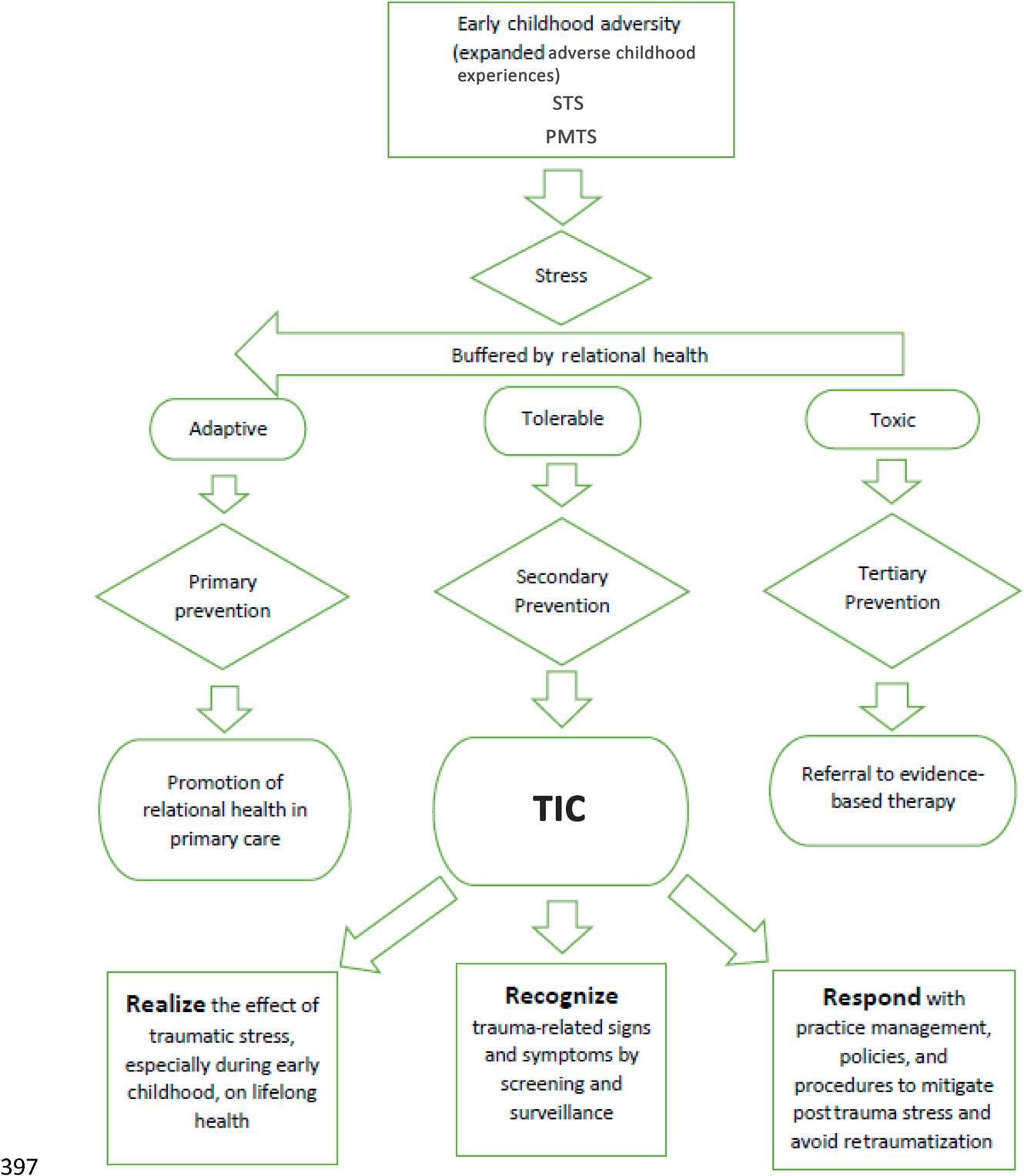
In a complimentary publication to Forkey’s AAP Clinical Report, a call for advocacy and a framework for policy changes for health systems was provided by Duffee. (Duffee et al, 2021) The figure below comes from this publication. In the figure STS refers to secondary traumatic stress and PMTS refers to pediatric medical traumatic stress. It outlines an algorithm that helps clarify actions clinicians can take to integrate a trauma-informed care model in their own practice settings. Current systems will need to innovate and adapt to bring about this necessary model of care.
Can being trauma-informed help those of us in the healthcare workforce personally as well as professionally ?
The answer is yes. According to the AAP clinical report, secondary traumatic stress among health care personnel may have many of the same long-term effects on health that affect children exposed to trauma. Some health care workers may also develop disabling post-trauma symptoms that can interfere with quality of life both at work and home. Health care workers may have their own trauma histories that contribute to their responses and feelings when exposed to the suffering of others. (Forkey, 2021) Physician suicides are occurring at alarming rates, with women doctors at exquisitely higher risk and incidence than their male counterparts. The mental health crisis remains significant, affecting many regardless of their station in life. As caregivers at work and home, the saying holds true. “You cannot pour from an empty cup.”
In the Caring Essentials Trauma-informed Professionals Certificate program, (Coughlin, Fuller, and DeWolfe, 2022) I have learned that it is possible to change from “ruined for good” to “recharged and ready to bring about good”. The course leaders from the Caring Essentials collaborative (Mary Coughlin, Kristi Fuller, and Tara DeWolfe) are intelligent, insightful, warm inspiring people. The program has encouraged me to reflect on thoughtful writings, inspiring talks, and testimonies of people who have reclaimed purpose in their professional and personal relationships using principles of trauma-informed care. I encourage you to find out more about trauma-informed care and to consider a training course for yourself and all the people with whom you share the meaningful vocation of clinical care. Thank you for allowing me to share this topic with you.
Be well.
Julie Lindower
Dr. Julie Lindower, MD MPH, is a newborn intensive care doctor at the University of Iowa Stead Family Children’s Hospital in Iowa City, Iowa. She views her work as an intentional effort to help create an environment in which children and their families can be healthy and live meaningful lives. She especially enjoys sharing the vocation of medicine with health professions students, who bring her a sense of hope for our collective future. You can find her on Instagram at @jlindowe.
Bibliography
Caring Essentials Collaborative. (2022, 10 30). Retrieved from Caring Essentials Collaborative: caringessentials.net
Duffee, e. a. (2021). Trauma-Informed Care in Child Health Systems. Pediatrics, 1-12.
Forkey, e. a. (2021, August). Trauma-Informed Care: AAP Clinical Report:Guidance for the Clinician in Rendering Pediatric Care. Pediatrics, 148(2), 1-26; e2021052580.
SAMHSA. (2022, 11 1). Retrieved from Substance Abuse and Mental Health Services: samhsa.gov
World Health Organization. (2022, November 1). Constitution of the World Health Organization. Retrieved from World Health Organization: https://www.who.int/about/governance/constitution
Works Cited
Forkey, e. a. (2021, August). Trauma-Informed Care: AAP Clinical Report:Guidance for the Clinician in Rendering Pediatric Care. Pediatrics, 148(2), 1-26; e2021052580.

